Medication-Assisted Treatment (MAT) on Long Island
Medication-assisted treatment combines FDA-approved medications with counseling to treat opioid and alcohol addiction — and it's the most effective approach modern medicine has. We connect Long Island residents with MAT prescribers across Nassau and Suffolk County, verify insurance coverage, and coordinate placement, often the same day you call.
What Is Medication-Assisted Treatment?
MAT uses medications like buprenorphine (Suboxone, Sublocade, Brixadi), naltrexone (Vivitrol), and methadone to stabilize brain chemistry, block the effects of opioids or alcohol, and relieve cravings — while counseling and support address the reasons behind the addiction. It is not "replacing one drug with another": these medications, taken as prescribed, don't produce a high. They give people the stability to work, parent, and rebuild. Federal agencies including SAMHSA and NIDA recognize MAT as the standard of care for opioid use disorder.
Comparing MAT Medications: Suboxone vs. Sublocade vs. Brixadi vs. Vivitrol vs. Methadone
The right medication depends on your substance history, how quickly you need to start, whether daily dosing fits your life, and what your insurance covers. Here's how the five options compare:
| Attribute | Suboxone (buprenorphine/naloxone) | Sublocade (buprenorphine XR) | Brixadi (buprenorphine XR) | Vivitrol (naltrexone XR) | Methadone |
|---|---|---|---|---|---|
| Treats | Opioid use disorder (OUD) | OUD (maintenance) | OUD (maintenance) | OUD & alcohol use disorder | OUD (heavy/long-term) |
| How it's taken | Sublingual film/tablet | Monthly SC injection (abdomen) | Weekly or monthly SC injection (4 sites) | Monthly IM injection | Daily oral liquid/tablet |
| Dosing frequency | Daily at home | Every 28 days in office | Weekly or monthly in office | Every 4 weeks in office | Daily at clinic (initially) |
| Time before starting | 12–24 hrs into withdrawal | ~7 days stable on oral buprenorphine | Weekly: after 1 test dose | 7–14 days opioid-free | Same-day admission at OTPs |
| Where you get it | Any waivered prescriber / pharmacy | Certified office visits | Certified office visits | Any qualified prescriber | Federally licensed OTPs only |
| Key advantage | Flexible, take-home, low barrier | No daily dosing decisions | Faster start, flexible dosing intervals | Non-opioid, no dependence, no taper | Highest retention for severe OUD |
| Considerations | Requires precipitated-withdrawal timing | Requires prior stabilization | Injection-site reactions | Full opioid-free window required first | Daily clinic visits at first |
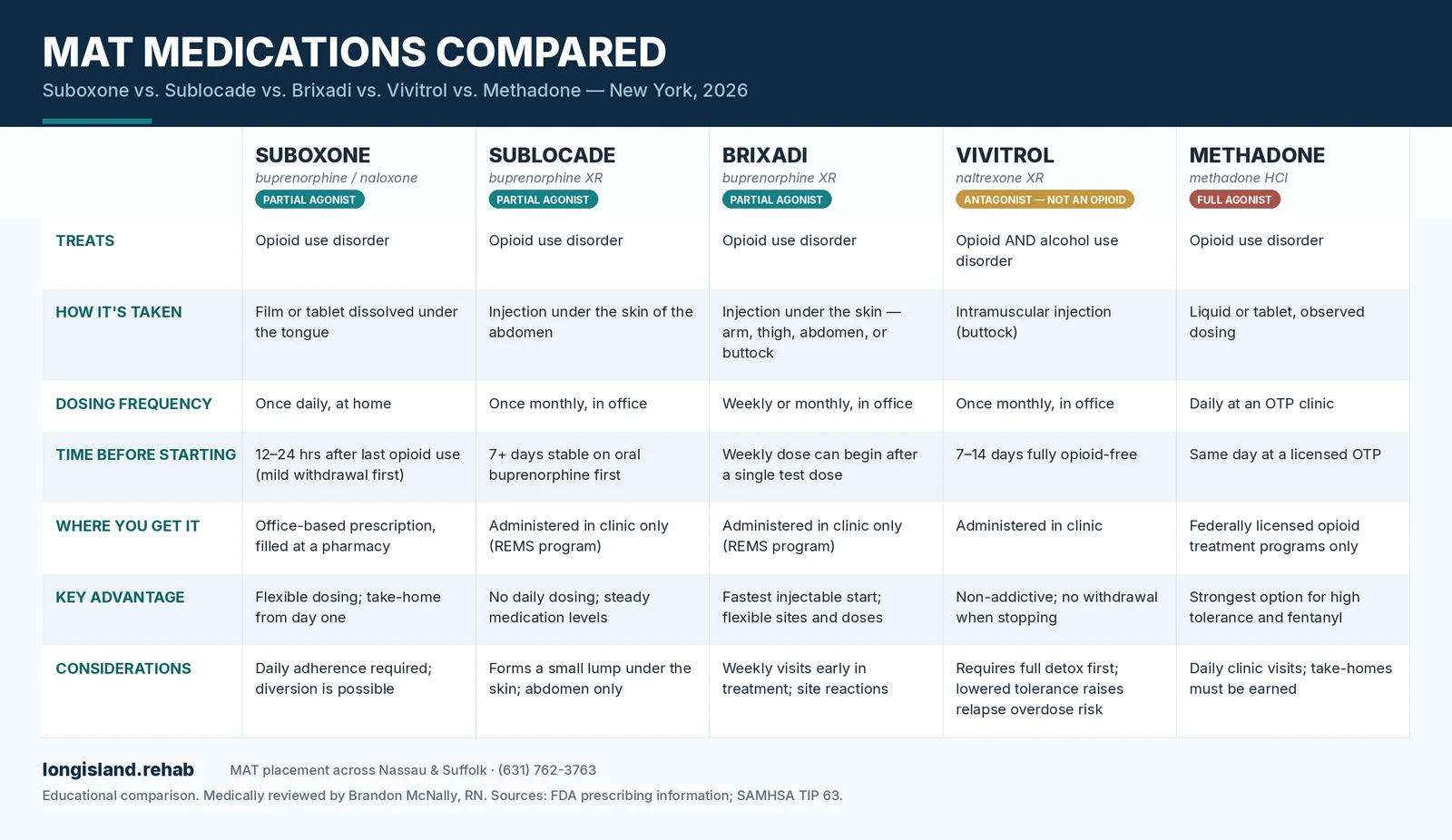
Key differences people ask about most: Brixadi vs. Sublocade — both are extended-release buprenorphine injections, but Brixadi comes in weekly and monthly versions, can be injected in four body sites, and the weekly dose can start after a single test dose, while Sublocade is monthly-only, abdomen-only, and requires about a week of stabilization on oral buprenorphine first. Vivitrol vs. buprenorphine options — Vivitrol is not an opioid at all, so there's no dependence and no taper, but you must be fully opioid-free for 7–14 days before the first injection. Methadone — the strongest option and often the best fit for heavy fentanyl use, but it's only dispensed through federally licensed opioid treatment programs with daily visits at first.
Find MAT Prescribers Near You on Long Island
If you've been searching for doctors that prescribe Suboxone near you or "Vivitrol providers near me," you've probably discovered the problem: directories are outdated, half the numbers don't answer, and the ones that do have month-long waits or don't take your insurance. That's the gap we close. We're not a clinic — we're navigators. We maintain current relationships with MAT prescribers across Long Island and match you based on medication, insurance, location, and how fast you need to start.
How matching works
- 1Call or message us
Tell us what you're using, what medication you're interested in (or let us walk you through the options), and your insurance.
- 2We verify and match
We confirm your coverage and identify prescribers with real availability — including same-week Suboxone inductions and clinics administering Sublocade, Brixadi, and Vivitrol.
- 3You start treatment
We coordinate the intake so you show up to a confirmed appointment, not a waitlist.
Nassau County
MAT prescriber placement in Hempstead, Levittown, Freeport, Hicksville, Long Beach, Valley Stream, and surrounding communities.
Suffolk County
MAT prescriber placement in Hauppauge, Brentwood, Islip, Smithtown, Riverhead, Patchogue, and across the county.
Is MAT Covered by Insurance in New York?
Almost always — and New York law is on your side. New York requires state-regulated commercial plans to cover medications for opioid use disorder without prior authorization for at least one formulary version of buprenorphine and for injectable naltrexone. NY Medicaid covers all FDA-approved MAT medications under a single statewide formulary, also without prior authorization. Where it gets complicated: Medicare splits coverage (office-administered injectables like Sublocade, Brixadi, and Vivitrol typically bill under Part B; take-home Suboxone films go through Part D), and self-funded employer plans regulated under federal ERISA law aren't bound by New York's mandates — coverage varies by plan.
| Plan type | Buprenorphine (Suboxone) | Injectables (Sublocade / Brixadi / Vivitrol) | Prior authorization |
|---|---|---|---|
| NY commercial (state-regulated) | Covered | Covered | Prohibited for formulary versions |
| NY Medicaid | Covered | Covered | Not required (statewide formulary) |
| Medicare | Part D | Typically Part B (office-administered) | Varies by plan |
| Self-funded employer (ERISA) | Usually covered | Varies | Plan-specific |
You don't need to figure out which category your plan falls into — that's part of what we do. We verify MAT benefits before matching you with a prescriber, so there are no surprise denials at the pharmacy counter.
How Much Does MAT Cost on Long Island?
With insurance, most people pay a copay per visit plus a prescription copay — often $0–$50/month for Suboxone under commercial plans and $0 under Medicaid. Without insurance, approximate cash ranges on Long Island are below. Manufacturer copay assistance (inSupport for Sublocade, Brixadi Copay Assistance, Vivitrol Co-pay Savings) can reduce out-of-pocket costs to as little as $0–$10 for eligible commercially insured patients — we help you enroll as part of placement.
- Cash: ~$60–$200/moInsured: $0–$50/mo copay typical
- Prescriber office visitCash: ~$150–$300Insured: Standard specialist copay
- Sublocade (monthly)Cash: ~$1,900–$2,000/injection listInsured: $0–$10 with inSupport copay assistance
- Cash: ~$1,900–$2,000/monthly-equivalentInsured: $0–$10 with Brixadi Copay Assistance
- Vivitrol (monthly)Cash: ~$1,500–$1,700/injectionInsured: $0–$5 with Vivitrol Co-pay Savings
How Effective Is MAT Compared to Detox Alone?
This is the most important question on this page, and the evidence is unambiguous. Detox alone — getting through withdrawal without ongoing medication — has high relapse rates for opioid use disorder, and the period right after detox is the highest-risk window for fatal overdose because tolerance drops while cravings don't — a risk especially acute with fentanyl and heroin. Treatment with buprenorphine or methadone is associated with roughly a 50% reduction in overdose death and all-cause mortality compared to no medication, according to research cited by the National Institute on Drug Abuse. People on MAT stay in treatment longer, use illicit opioids less, and are more likely to keep jobs and custody of their children. SAMHSA's TIP 63 guidance is blunt about it: medication is the standard of care for opioid use disorder, and withholding it isn't a more "pure" form of recovery — it's a riskier one.
MAT works best when paired with structured care. Many people combine medication with intensive outpatient therapy, and those with more severe use histories often start in inpatient rehab before stepping down to ongoing MAT.
Authority sources: NIDA — Medications for Opioid Use Disorder · SAMHSA TIP 63.
Is MAT Safe During Pregnancy?
Yes — and it's strongly recommended over detox. For pregnant women with opioid use disorder, buprenorphine or methadone is the standard of care endorsed by ACOG and SAMHSA. Attempting withdrawal during pregnancy carries risks of relapse and overdose that endanger both mother and baby, while stable MAT is associated with better prenatal care engagement and healthier birth outcomes. Newborns may experience treatable neonatal abstinence syndrome, which hospitals on Long Island manage routinely — it is not a reason to avoid treatment. Vivitrol is generally not started during pregnancy. If you're pregnant and using opioids, this is a same-day placement priority for us: call and we'll connect you with prescribers experienced in perinatal MAT.
Frequently Asked Questions About MAT
Getting Started
Do I need to be in withdrawal to start Suboxone?
Can I start MAT the same day I call?
Can I get MAT through telehealth in New York?
What is the Suboxone 3-day rule?
Medications & Safety
Is MAT just replacing one addiction with another?
What are the side effects of MAT medications?
Can I drink alcohol while on MAT?
How long do people stay on MAT — and can I taper off?
Does MAT reduce the risk of overdose?
Coverage & Daily Life
Which insurance plans cover MAT in New York?
Can I keep my job while on MAT?
Does MAT show up on a drug test — and can employers see it?
Same-day placement calls answered 24/7
Talk with a navigator now to match with a Long Island MAT prescriber and verify your insurance.
Call (631) 762-3763Related Resources
Medical References & Sources
This page contains information sourced from peer-reviewed medical literature, federal health agencies, and accredited medical institutions to ensure accuracy and compliance with E-E-A-T (Experience, Expertise, Authoritativeness, and Trustworthiness) standards.
- Substance Abuse and Mental Health Services Administration (SAMHSA). "Medications for Substance Use Disorders." SAMHSA. Available at: https://www.samhsa.gov/medications-substance-use-disorders
- National Institute on Drug Abuse (NIDA). "Effective Treatments for Opioid Addiction." NIH. Available at: https://nida.nih.gov/publications/effective-treatments-opioid-addiction
- National Academies of Sciences, Engineering, and Medicine. "Medications for Opioid Use Disorder Save Lives." The National Academies Press, 2019. Available at: https://nap.nationalacademies.org/catalog/25310/medications-for-opioid-use-disorder-save-lives
- Mattick, R.P., Breen, C., Kimber, J., & Davoli, M.. "Buprenorphine maintenance versus placebo or methadone maintenance for opioid dependence." Cochrane Database of Systematic Reviews, 2014 DOI: 10.1002/14651858.CD002207.pub4. Available at: https://doi.org/10.1002/14651858.CD002207.pub4
- Sordo, L., Barrio, G., Bravo, M.J., et al.. "Mortality risk during and after opioid substitution treatment: systematic review and meta-analysis." BMJ, 2017 DOI: 10.1136/bmj.j1550. Available at: https://doi.org/10.1136/bmj.j1550
- American Society of Addiction Medicine (ASAM). "National Practice Guideline for the Treatment of Opioid Use Disorder." ASAM, 2020. Available at: https://www.asam.org/quality-care/clinical-guidelines/national-practice-guideline
- New York State Office of Addiction Services and Supports (OASAS). "Medication-Assisted Treatment (MAT)." OASAS. Available at: https://oasas.ny.gov/mat
Medical Disclaimer
The information provided on this page is for educational purposes only and should not be considered medical advice. This page does not provide medical diagnoses, treatment prescriptions, or clinical recommendations. Always consult with qualified healthcare professionals for diagnosis and treatment of substance use disorders. If you are experiencing a medical emergency, call 911 immediately.
This content was written by certified addiction professionals and reviewed by licensed medical practitioners to ensure accuracy and adherence to current clinical guidelines. Last fact-checked: November 2026.
If you or someone you know is struggling with substance use, you can reach our 24/7 confidential Long Island Rehab Helpline at 631-762-3763 for free, confidential information and treatment referral.